During stressful times we tend to focus on the challenges and the struggles. It is important to not lose sight of the positive in our lives and to give gratitude.
Over the past few weeks, I have witnessed many amazing people stepping up to help everyone. Thank you, Sue Jones and Kelly Hassall, for your ongoing dedication and leadership to help RTs through Respiratory Therapy Society of Ontario (RTSO). Thank you, Gino Luigi De Pinto and Sue A., for keeping the RTSO website up to date with the latest resources.
Thank you, Thomas Piraino, for putting together the great resource on your website, and answering questions live on social media.
Also, a big thank you to Carolyn McCoy, Andrew West, Carole Hamp and Kevin Taylor for your ongoing hard work in the background.
Thank you to RT programs for lending your ventilator to hospitals, and taking your third-year students out of clinical rotations to keep them safe.
Farzad Refahi March 23, 2020 www.Respiratory.Blog/gratitude/ [End]
I have heard this question many times and in various forms.
Who is a respiratory therapist? What do respiratory therapists do? Where do respiratory therapists work?
With the current COVID-19 situation, respiratory therapists have been mentioned frequently. This blog post is meant to be a very quick overview. If you have any questions feel free to contact me and get in touch with your respiratory therapy organizations. I usually write for clinicians, but this post is meant for everyone as everybody is impacted by COVID-19.
Who are respiratory therapists?
“Respiratory Therapists are health care professionals who monitor, assess and treat individuals who have difficulty breathing”
How and why was the profession of respiratory therapy initiated?
The origin of this profession is from the second world war. It began as a technician role to reduce the workload of physicians and nurses. With a focus on the cardio-respiratory system, the role has evolved into a therapist and now includes various responsibilities.
What are the roles and responsibilities of respiratory therapists?
To keep things simple, I am going to give you a few different scenarios. They are not referring to any specific patient or organization. The teams are made of many amazing and dedicated clinicians who will be omitted in these scenarios so we can focus on the RT role!
Here are three scenarios to put things in perspective:
Case One: Asthma Exacerbation
Mary, and her parents, had felt that her asthma was not fully controlled for a few days and the recent cold has made her breathing much more difficult. Today her mother took her to an emergency department (ER) due to the severity. In the ER, a respiratory therapist is called to initiate the nebulized Salbutamol and to re-assess the patient. Despite various interventions, Mary continues to deteriorate and the decision is made to assist Mary’s breathing with the use of a ventilator. An RT places a breathing tubing in the trachea and attaches it to a unit that breathes for the patient (i.e. a ventilator). The RT continues to monitor and adjust the ventilator to optimize Mary’s breathing. When Mary’s condition improves, assistance from the ventilator is discontinued and the breathing tube is removed. Mary is now able to breathe on her own. Part of the discharge process, an RT sits down with Mary and her parents to discuss self-assessment and monitoring, and proper inhaler techniques. A follow-up appointment, in a couple of weeks, is scheduled for Mary at the Asthma Clinic. In the Asthma clinics RTs perform a breathing test, called Spirometry, and provide patient education which includes understanding the disease, management, prevention and optimization in case things don’t feel like the norm.
Case Two: COPD Exacerbation
Michael ignores the worsening of his cough, chest tightness and difficulty breathing with even short distance walks. Today he finally decides to consult his family doctor. A decision is made for him to visit an ER. In the emergency department, various tests and treatments are done, and an RT is called to start supporting Micahel’s breathing (using a mask and a supportive unit called BiPAP). Michael’s breathing is optimized over the next day. He is transferred to the general ward for monitoring. Before discharge, an RT meets with Micahel for a smoking cessation conversation. The RT also provides education about the need for ongoing oxygen. A follow-up Pulmonary Function Testing and respirologist/pulmonolgist consult are scheduled. An RT with a Home Oxygen Company/team would visit Michael to set up the equipment, perform assessments, and provide further education. During Pulmonary Function Testing, an RT walks Michael through various breathing tests. At the respirology/pulmonology visit, an RT may sit down with Michael to review the proper inhaler technique. Same RT may also provide a smoking cessation consult. A follow-up PFT and respirology/pulmonology visit are scheduled.
Case Three: Mona and Baby Lisa – Labour and Delivery
Based on the assessments and monitoring of Mona, a difficult delivery is suspected. The team, including a respiratory therapist, is present in the delivery or operating room. Immediately after birth, RT and nurses perform the routine assessments and provide the required care. In this example, the RT puts a small “mask” on Baby Lisa’s nose to deliver a small amount of airflow or pressure. This will help to keep the lungs open slightly longer, and in turn, make breathing easier for Baby Lisa. The RT, part of the team, transfers Baby Lisa to the intensive care unit for further monitoring. Baby Lisa’s breathing is optimized by adjusting the CPAP unit as required. Use of CPAP will be weaned off as Baby Lisa starts feeling better. If Baby Lisa requires even more support, the RT can use a breathing tube to establish a better pathway, and a ventilator to deliver a more controlled breathing support.
There is more…
Respiratory therapists are involved with other roles such as managers, researchers, teachers, inventor, remote support using the phone/video-chat, transport team, consultant, policymaker, in-hospital code blue/pink resuscitation teams, operating rooms, sleep labs, CPAP educators, and others.
What can an RT do for someone with COVID-19?
Respiratory therapists can be part of the team who does the initial assessment. By applying nasal prongs or a mask, an RT can improve the body’s oxygen levels. When needed and indicated, inhalers can be given to optimize breathing. Assistance in breathing can be provided using non-invasive, such as CPAP and BiPAP, and invasive measures (Ventilators).
How to become a respiratory therapist?
Most clinicians in Canada complete their undergraduate studies and then apply for one of the many respiratory therapy programs in Canada. For the list of available programs in Canada, I will refer you to the website of the Canadian Society of Respiratory Therapists: https://www.csrt.com/rt-profession/#education. The training usually involves two years of academic and simulation learning, and a final year of clinical placements.
How much do respiratory therapists get paid?
Based on Payscale.com, the median hourly rate is $31.80 in Canadian dollars ( as of March 22, 2020, https://www.payscale.com/research/CA/Job=Respiratory_Therapist/Hourly_Rate ). As you can guess, the pay is higher with more years of experience, and with roles that entail more responsibilities and that in the acute care settings.
Where can I get more information about respiratory care and respiratory therapists?
On the national side, visit the Canadian Society of Respiratory Therapists: www.CSRT.com.
On the provincial side visit the College of Respiratory Therapists of Ontario: www.CRTO.on.ca, and Respiratory Therapy Society of Ontario: www.RTSO.com.
On a personal RT perspective, there is my website: www.Respiratory.Blog . In my interviews with different respiratory therapists, I try to share different perspectives and insights. Here is one example: Mieke Fraser’s post at http://respiratory.blog/mieke/ (published on October 25, 2017).
Thanks for your interest in respiratory care and respiratory therapists! Share this with others who may find it helpful!
Stay safe. Frequently wash your hands. Practice social isolation.
Here is a PDF version of this post for ease of sharing:
Today is March 20th, 2020. The first day of spring. Happy Nowruz to all those who celebrate the new year. Iranians, among few other nations, have the first day of spring as their new year.
While new year celebrations involve visiting others and sharing delicious food, this year will be quiet. I hope it is quiet. Let’s continue the social isolation. Let’s continue to practice proper hand hygiene. Let’s self-isolate if you are feeling unwell. Let’s think about the vulnerable population and the elder members of the family.
My blog posts are usually meant for clinicians. This time, I am writing to every one, since dealing with COVID-19 is beyond the work of clinicians and healthcare system.
While you monitor your physical health, please don’t forget about your mental health. There are various electronic and video communication options that allow you to connect with others. Call the elderly to check-up on them. If you know someone in isolation, ask if they require groceries (being dropped behind their door).
Those who experienced SARS in 2003 may experience higher levels of anxiety around this time (especially clinicians). Make sure you connect with proper resources, support and intervention if required.
Give yourself mental breaks. Find a few trusted sources for news and COVID-19, and only review those. Constantly reading about it may induce increased anxiety. ( www.RTSO.ca is one of my trusted sources.)
Find appropriate stretches and exercises that can be safely done at home. Stay hydrated. Use this opportunity to stop smoking. Pick up that book that you always intended to read!
Don’t forget about the positive. Give gratitude for the good in your life. There are many great people who are doing their best to help out. A quick shout out to respiratory therapists and clinicians who continue to work to keep us healthy. Fatima Foster is creating a supportive online community for clinicians who are experiencing some anxiety around this time. John Meloche from Melotel Inc. is using the resources in his company to support communities and organizations who have non-for-profit COVID-19 support groups. There are many more examples if you look for them!
Our Pulmonary Function Lab has been closed for the past two days to reduce the risk of transmission to patients, especially the vulnerable populations. Things are changing daily, and there many unknowns. (To non-clinicians reading this, we do know proper hand hygiene and social distancing works!)
I have worked full time in a PFT setting over the past 5 years. With PFT lab closed, and a chance for deployment to other units, I need to do some reviewing!
The Essentials of Respiratory Care by Robert M. Kacmarek .Fourth Edition. 2005. Elsevier Mosby
The Essentials of Respiratory Care, Fourth Edition, by Robert M. Kacmarek, Steven Dimas and Craig W. Mach is one of my resources. This textbook was not actually a resource during my studying, however, it was a recommendation by one of the instructors (shout out to Paul Smith at The Michener Institute). Since I have not been trained in the acute care setting of my hospital, I don’t know about many of the protocols, selection of equipment and policies. I am still going to use this opportunity to review some respiratory care knowledge.
Do you have any up to date, open access and free resources to recommend?
Hearing About Flattening The Curve While Listening to Dr Mike on YouTube As He Discuss Coronavirus.
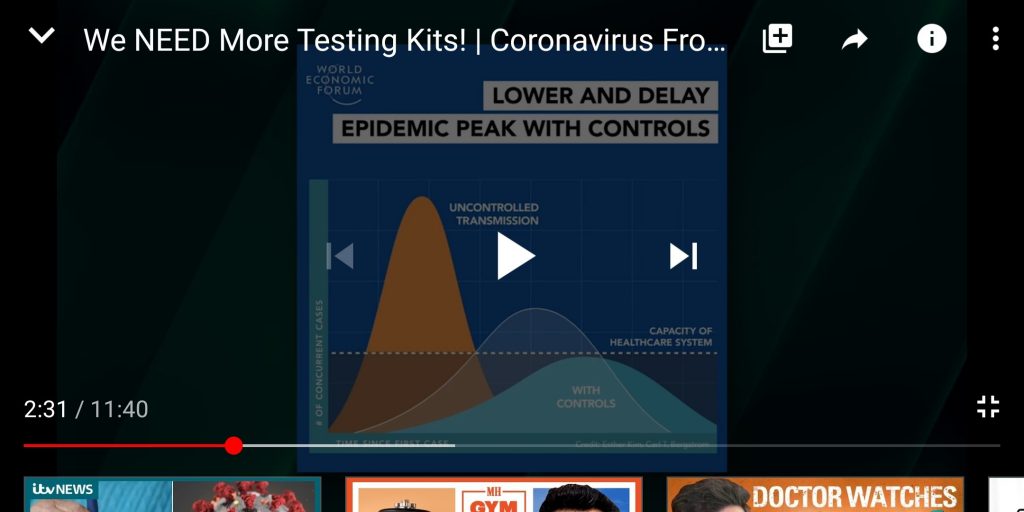
I try to get information from multiple sources online. One of these sources is Dr Mike who is a family physician in the United States. In one of his latest videos titled ‘We NEED More Testing Kits!’, I came across a concept which I had forgotten about. At 2:10/11:40 he quickly refers to ‘Flattening The Curve’:
… Here in United States, we simply do not have enough ICU beds if everyone is to get this virus simulatenously, so by slowing the rate at which this virus infects others we doing “Flattening the Curve”
A large number of people using limited resources at the same time will saturate and overwhelm the system. The system can provide better care if the same number of people access these resources over a longer period of time (versus all at once).
When it came to public health, disease prevention and elimination of spread were at the core of my thoughts. Now I have learned that slowing the spread of disease is not necessarily a total defeat. Even a slow down, is a success in better access to care (in the highly contagious disease when total isolation and zero spread is unrealistic).
You can watch the full video using the link below:
Link to Dr Mike’s video published on Mar 15, 2020 https://youtu.be/DfMl6W6N7-A , watched by Farzad Refahi on Mar 15, 2020
As healthcare providers, we can better educate the public about the nature of the disease and proper hand hygiene. Also, we can encourage unnecessarily gathering of people in public spaces. As a group, we can look after the vulnerable population.
On a personal note, my wife, who is feeling fine, cut her business trip short due to the quickly evolving situation with COVID-19. I purchased food and supplies to last her at least two weeks. I left for my parents before her taxi got to our place. She has decided to follow the recommendation of self-isolation for two weeks. We are lucky that my parents live close by and are more than happy to have me for the two weeks. Of course, it is not easy being apart even longer than planned, however it is a small price to pay for the greater good (especially when as an RT, I have face to face interactions with patients at work).